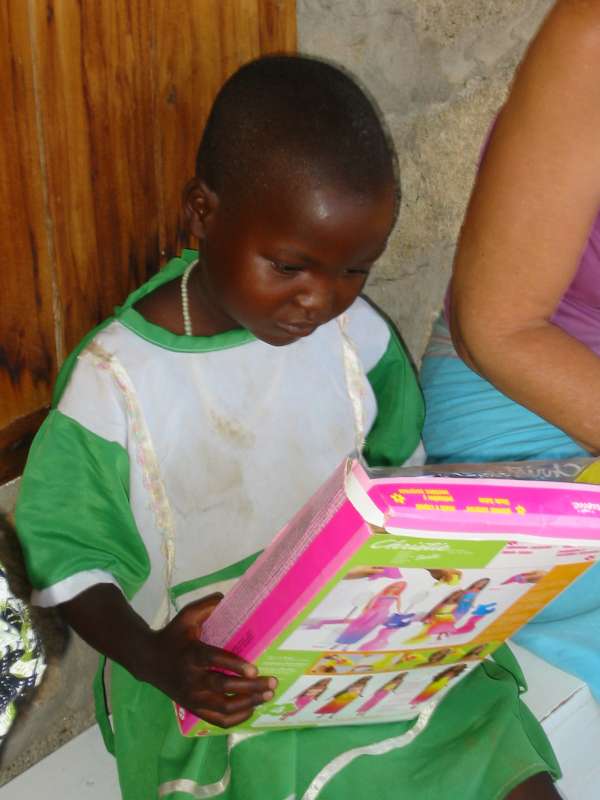
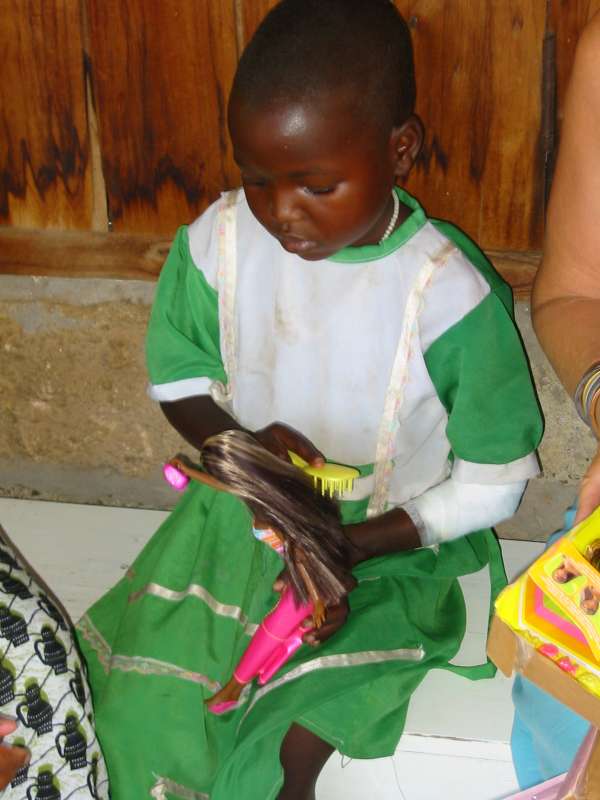
Chemandazi receives the Barbie doll gift
Private homepage – Hans-Georg Michna
Kenya travel reports: 1999, 2000, 2002, 2003, 2004, 2005, 2006, 2007, 2008, 2009, 2010, 2011, 2012, 2013-Goma, 2013, 2014, 2015, 2016, 2017, 2018, 2019
Epilogue – Chamandazi goes home
HANS-GEORG MICHNA
Please click on the small pictures to see the full-size pictures.
Photos and copyright © 2002-2003 Dr. Elizabeth Meyerhoff-Roberts,
Copyright © 2004-2023 Hans-Georg Michna.
Photographer 2003: Rashi Gupta
A few readers had the problem that after clicking on a picture, then going back to the main page, all thumbnail pictures were reloaded. This is typically caused by Internet Explorer cache corruption. It can often be repaired by going to the Internet options and deleting the temporary Internet files.
In 2002 Chemandazi received a gift of a Barbie doll. For a Pokot child, as for many Kenyan children, toy dolls are not common, and they wouldn't know what to do with them. Chemandazi had to be shown how to play with a doll.
Chemandazi receives the Barbie doll gift
During treatment, Chemandazi's arm looked like this. If you remember the pictures in the 2002 travel report, you can see the progress. For a while the people treating her were seriously worried whether she would survive the cobra bite at all.

Chemandazi's arm during treatment
Chemandazi received skin grafts which now cover most of the large wounded area on her arm and hand.


After receiving skin grafts
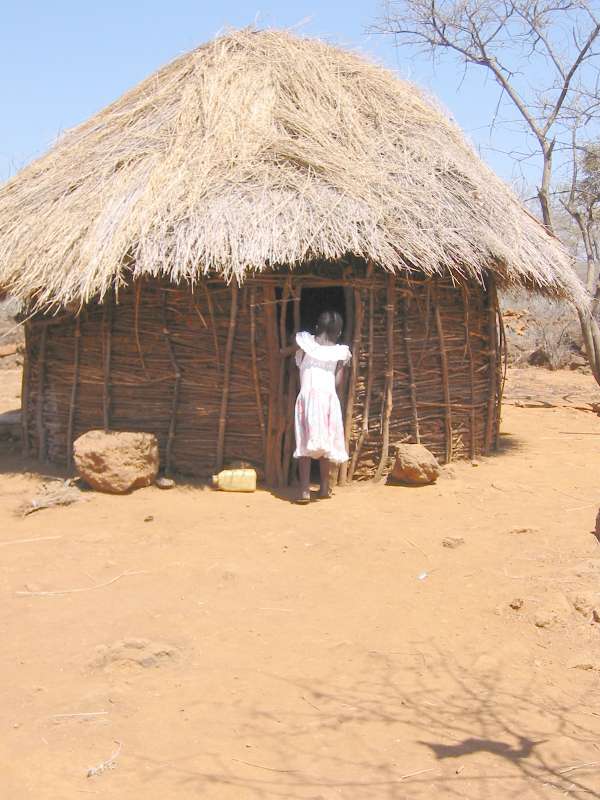
After her successful treatment including the skin grafts, Chemandazi eventually had to be taken home, which means many miles into the semiarid countryside of central Kenya, back to her mother.
Chemandazi had been in contact with a different culture, one she would not by then have experienced without the cobra bite. She was dressed in European-style clothes, rather than the traditional Pokot outfit, which for children means almost nothing. For her, the return home meant going from regular good food and the foreign lifestyle back to the life of the Pokot in the countryside.


Looking back to Lake Baringo from the north
















Inspecting the site on her leg where the skin grafts were taken from, and her hand




The woman on the right is Chemandazi's mother.





The man is, to the best of my knowledge, not Chemandazi's biological father.



Being with her little brother again



By luck I met Chemandazi in Baringo when she was coming in for some treatment at the RAE Dispensary.



Chemandazi's arm
Her left arm and hand are much better now. She regained nearly unimpeded use of both.
Unfortunately even at a renowned hospital the treatment was less than perfect (due to such hospitals being overrun by patients, having to treat hundreds every day). They put her arm in a cast for a month. Had the cast really stayed on for that time, the consequences might have been horrible, as one of the stitched areas broke open and now forms another wound. Fortunately at the RAE Trust clinic they noticed that, took the cast off, and the wound should now heal.



She's a happy girl now.
In closing I'd like to remark that the thanks for Chemandazi's recovery goes mainly to the RAE Trust dispensary in Baringo, in particular to Dr. Elizabeth Meyerhoff-Roberts, and of course to the people who donated money to this good cause. Without these people Chemandazi would almost certainly not have her usable arm now, the arm would likely have been amputated, and she might have died even before that.
However, there are many cases like Chemandazi, and few are as lucky as she was.
A small dispensary, located in a remote area of Kenya’s Rift Valley, has developed a new approach to the successful treatment and follow-up of burns in a rural African setting. The dispensary has become an integral part of the RAE Trust’s multi-faceted community development programme. For over 15 years, the Rehabilitation of Arid Environments (RAE) Trust has worked closely with the impoverished local communities of the semi-arid Baringo lowlands to improve their livelihoods. Appropriate land reclamation, techniques and community based strategies have been developed to transform degraded drylands into productive rangelands sustained and managed by the local people themselves.
The Work of the RAE Dispensary has been defined entirely by the needs of the community. It began over 15 years ago with women seeking help for themselves and their children in the treatment and follow-up care of skin infections, wounds, sores and tropical ulcers which are prevalent in the area. Today, the dispensary plays a valuable role in the treatment of external wounds and specialises in treating burns. The dispensary also promotes and provides a family planning service, as well as educating the community about primary health care issues, hygiene and AIDS.
Elizabeth Meyerhoff supervises and manages the dispensary with the assistance of Anna Owuor, a woman from the local community who has had some training from Marie Stopes International but has been trained mainly on-site by Elizabeth. Elizabeth herself is self-trained through reading and years of experience. She has lived and worked in rural areas of Kenya for some 30 years. Originally from California, she began helping people who urgently needed treatment but had nowhere to turn for help while she was carrying out research among the Pokot people of remote north-western Kenya. After receiving her PhD in Social Anthropology from Cambridge University, UK, she returned to Baringo in Kenya to co-manage the RAE Trust with her husband, Murray Roberts.
The local Baringo people live an unsophisticated lifestyle without access to running or clean water or electricity. Many of the older people are unable to read and write and have little or no knowledge of hygiene and sanitation. This is slowly changing with the education of the younger generation. However, this in turn can have detrimental consequences for the health of the local children. With most of the older children going to school, there is no one to help with herding and other domestic tasks, leaving the mothers so busy that they are unable to care for their large families. Small babies are minded by very young siblings, resulting in large numbers of accidents, especially burns.
Many of the patients treated at the RAE Dispensary are children, some of whom walk up to 40 kilometres to receive assistance and treatment. Adherence to basic principles of wound management and individual follow-up treatment and care are the key to the success of the RAE clinic. The dispensary co-operates fully with the government and mission health care facilities in the Baringo lowlands, but these facilities are very limited and most lack medical supplies and fully qualified personnel. The staff do not emphasise follow-up care, and the patients are not given clear instructions about taking their antibiotics. As a result, infections are often not cured and resistance develops.
RAE is prepared to assist all burns cases initially but is aware of its limitations. Sometimes referral of difficult cases to more comprehensive facilities outside the immediate area is essential, and RAE can assist with organisation, transport and cost sharing. In turn, other facilities in the area refer patients to RAE for long term follow-up treatment and holistic care.
Elizabeth Meyerhoff uses Sofra-tulle gauze on broken/infected areas, covered with a mix of locally purchased tetracycline cream and Vaseline. Moisture and warmth are maintained by covering this with silver paper (in many instances she uses silver paper from inside cigarette cartons spliced together) and this is held in place by a simple gauze bandage. Tegaderm dressing would be more effective and simpler to use but it is not available locally, and the cost of importing it would be prohibitive. In addition to keeping the wound moist and warm, RAE seeks to supplement inadequate diets with essential vitamins to aid repair.
Patients are made aware that they are responsible for attending the clinic as instructed. During treatnient, simple explanations are constantly reiterated. On occasions arrangements have been made for patients to lodge locally in order to receive treatment regularly over a long period of time. Occasional home visits are undertaken (transport permitting) when patients arc unable to reach the clinic.
It would be virtually impossible to maintain the sterility necessary for treatment of burns in a rural home situation, given the dusty and unhygienic conditions, where children often sleep on the floor of a hut with goats. The patients must, therefore, return to the clinic for regular followup treatment. The approach developed at RAE allows patients to be treated every other day, going home for a full day and returning to the clinic with the burn still covered and clean under the silver paper. The fact that they can be treated as out-patients helps them to heal quickly and reduces costs. There are, of course, times when good progress in healing is hampered or ruined by the patient not following instructions carefully, missing appointments or ceasing to visit the clinic before being totally healed. In such cases, an attempt is always made to visit the patient at home and encourage the family to restart the treatment.
RAE does not normally charge for treatment as most people of the area are poor and the aim is to serve as many people as possible. Occasionally, when costs for an individual case run into tens of thousands of Kenyan Shillings, some contribution is sought towards the cost of medicines and dressings used. Sometimes a local fund raising occasion, organised by the people themselves, takes place to cover this. Donations are also received from various sources.
Over a twelve month period 1998/99, 202 patients made a total of 484 visits to the RAE Dispensary to receive advice, diagnosis, treatment and follow-up care. Of these, 39 were burns cases, ranging in severity from relatively superficial to very severe burns, some of which later required grafting.
The RAE Clinic continues to be an important community facility, particularly for women and children of the area. The Clinic is open three times a week, and treats mostly burns, wounds and skin infections, as well as providing reproductive health care services, in total, some 700 people were seen by the Clinic over the last project year. The majority of these, an approximate 615, were health care clients, with burn patients returning multiple times for treatment. The Clinic is well known throughout the basin for its success in healing even severe burns with little scarification. People come from many miles away knowing that careful and successful treatment for burns is not available elsewhere in the District. In some ways, the reputation of the RAE Clinic has grown larger than the facility itself. A few extensive full depth burns had to be referred to larger Hospitals this past year. In addition to the positive collaboration the Clinic enjoys with local health facilities, especially Marigat Mission Health Centre, new alliances were consolidated with the Bethany Crippled Children’s Centre and AIC Hospital in Kijabe. This made it possible to send a number of patients needing skin grafting and straightening of contracted limbs for further treatment. In March 2003, additional cooperative links were established with doctors and interested individuals in California when the RAE Social Scientist gave a presentation about the RAE Clinic.
An additional 85 women clients visited the RAE Clinic for reproductive health care services over the project year. After counselling and examination, these women were provided with a variety of different family planning methods of their choice. Family planning has become more openly accepted in the Baringo basin over the years, and client numbers are steadily increasing. There were 45 new clients this project year, many of them younger women who opted for longer term family planning methods. On 30 April 2003, the Marie Stopes International outreach team came and inserted 25 Norplant (a five year family planning method), and completed one tubal ligation. Due to the growing number of requests for Norplant, in particular, plans have been made for Marie Stopes to return to the RAE Clinic again later this year. Over August 2003, the RAE Nurse completed a three week course in Nairobi given by Marie Stopes where she received practical and theoretical training in reproductive health care. Her training will greatly assist her in promoting and providing appropriate, updated services to the women of Baringo.
The RAE Nurse was also trained in HIV/AIDS awareness building over the last project phase. From May to June 2003, the RAE Nurse and other extension staff visited eight local primary schools to educate and create awareness about the growing problem of HIV/AIDS in Baringo. The main topics covered were the definition of HIV and AIDS, mode of transmission, means of transmission, prevention and current statistics. Simple extension materials were created for the interactive presentations that reached over 490 students in Standards 6, 7 and 8. In addition to posters and flip charts, drama was used with role cards to assist the short plays presented by students. Open discussions and questions were encouraged after all the presentations, but responses varied from school to school. In general, it was found that the students in schools closer to towns (such as Kampi ya Samaki Primary School) were more willing to discuss their questions and fears openly, compared to students from more rural schools (such as Loberer Primary School) who often remained quiet letting their teachers respond for them. RAE will work towards fulfilling the request from schools for this programme to be expanded, as well as linking the programme to other HIV/AIDS awareness building efforts being carried out.
If you find typos, orthographic errors (even small ones), ungrammatical sentences, wrong or illogical information in this text, or if you want me to write more details about something in particular, please click on the email sign below and write to me. Many thanks!
Photos and copyright © 2002-2003 Dr. Elizabeth Meyerhoff-Roberts,
Copyright © 2004-2023 Hans-Georg Michna.
Photographer 2003: Rashi Gupta
Private homepage – Hans-Georg Michna
Kenya travel reports: 1999, 2000, 2002, 2003, 2004, 2005, 2006, 2007, 2008, 2009, 2010, 2011, 2012, 2013-Goma, 2013, 2014, 2015, 2016, 2017, 2018, 2019

hits since 2007-11-01
Free PHP scripts by PHPJunkYard.com